How to Master Nurse Charting & Avoid Mistakes


In this article
Embarking on a career in nursing can give rise to feelings of excitement, anxiety, and overwhelm. There’s a lot that goes into patient care, and you’re expected to keep track of everything in each patient’s chart. Writing nursing notes throughout your day can seem tedious, but are essential and will become second nature with time.
What is charting in nursing
A patient’s chart keeps track of their vitals, medications, and procedures. Basically, it’s a living record of their medical care over time and it is cumulative. Patients don’t get new charts with each visit. Instead, their existing chart is updated with new information from each encounter with a specific provider. Different healthcare entities don’t usually update the same records. For example, most patients have separate charts at the clinic where they see their primary care provider and the hospital where they seek emergency medical services.
Even though doctors, nurse practitioners, and other autonomous medical professionals write the majority of patient notes, nurses have a crucial role in charting. Anytime a nurse checks a patient’s vitals, gives a medication, or provides other patient care, they document their interaction in the patient’s chart.
How does charting help protect you?
Charting is one of the biggest ways to protect yourself as a nurse. In the healthcare world there is a saying, “If it isn’t charted then it wasn’t done. When hospital management or a legal team is searching through a patient’s file to discover how an injury or death occurred, they will look at everything that was charted. If pieces are missing you could be held liable.
Legal Nurse Donna Schisler recommends “all medical staff to over chart. Fill out all the required charting, and then write notes. When something significant is happening with your patient, write multiple notes and use as much detail as possible. If we can see that you followed orders, caught mistakes, expressed concerns, fought for your patient, and were attentive, then you will generally be safe from repercussion. If you did not chart well and a lawsuit occurs four years later, where we ask you to detail your care for one of your 2000 patients during that time, you will most likely be unable to do so. Charting is time-consuming, but in the end, it is your best friend.
- Highest-paying states and cities, ranked from live contracts
- Take-home pay and tax considerations
How do you avoid medical mistakes?
Donna Schisler draws from her RN experience and found that making the following practices standard and notating them down will help nurses and healthcare professionals protect their license.
- Use the MAR to verify a medication is to be given to your patient.
- Ensure pharmacy has approved the medication.
- Use the dispensing device correctly – search using both generic and brand name. If that is unsuccessful, ask another nurse, charge nurse, or pharmacy how to find the correct medication.
- Use the scanner to verify the right medication is being given to the right patient.
- Look at the medication you are giving. Make sure there are no errors or warnings that were missed. Ensure instructions for administration are followed.
- Verify the patient’s name and DOB and explain what you are giving them.
- If you have questions, are unable to find a medication, or are giving something with which you are unfamiliar, reach out to another nurse, a charge nurse, or pharmacy. This act alone could save a life.


Healthcare professionals used to use paper charts to keep track of patient records. Every note was handwritten, and it was especially difficult to share records with both patients and other providers since they would need to photocopy each page.
Healthcare technology has revolutionized the way clinicians keep patient records. Most clinics, hospitals, and other facilities transitioned to electronic medical records (EMR) in the last couple of decades. There are so many different nursing charting systems to choose from, that interoperability has become the latest challenge with patient records.
Different EMRs can’t communicate with each other, so sharing patient records can still be a cumbersome process despite the switch from paper to software based systems. Healthcare professionals also need extensive training to learn the ins and outs of a new EMR system. So, it’s important for nurses to have a formula for charting that can ease their transition should they seek employment at a facility that uses an EMR system they are unfamiliar with.
How to write a nursing note
Writing nursing notes should be nearly second nature once a nurse graduates from nursing school. It should be a routine part of your workflow that you do almost automatically, like washing your hands as you enter a patient’s room. If you’re not sure how to write your nursing notes, you may benefit from learning the SOAP note method.
What is the SOAP note method?
SOAP noting contains four main components:
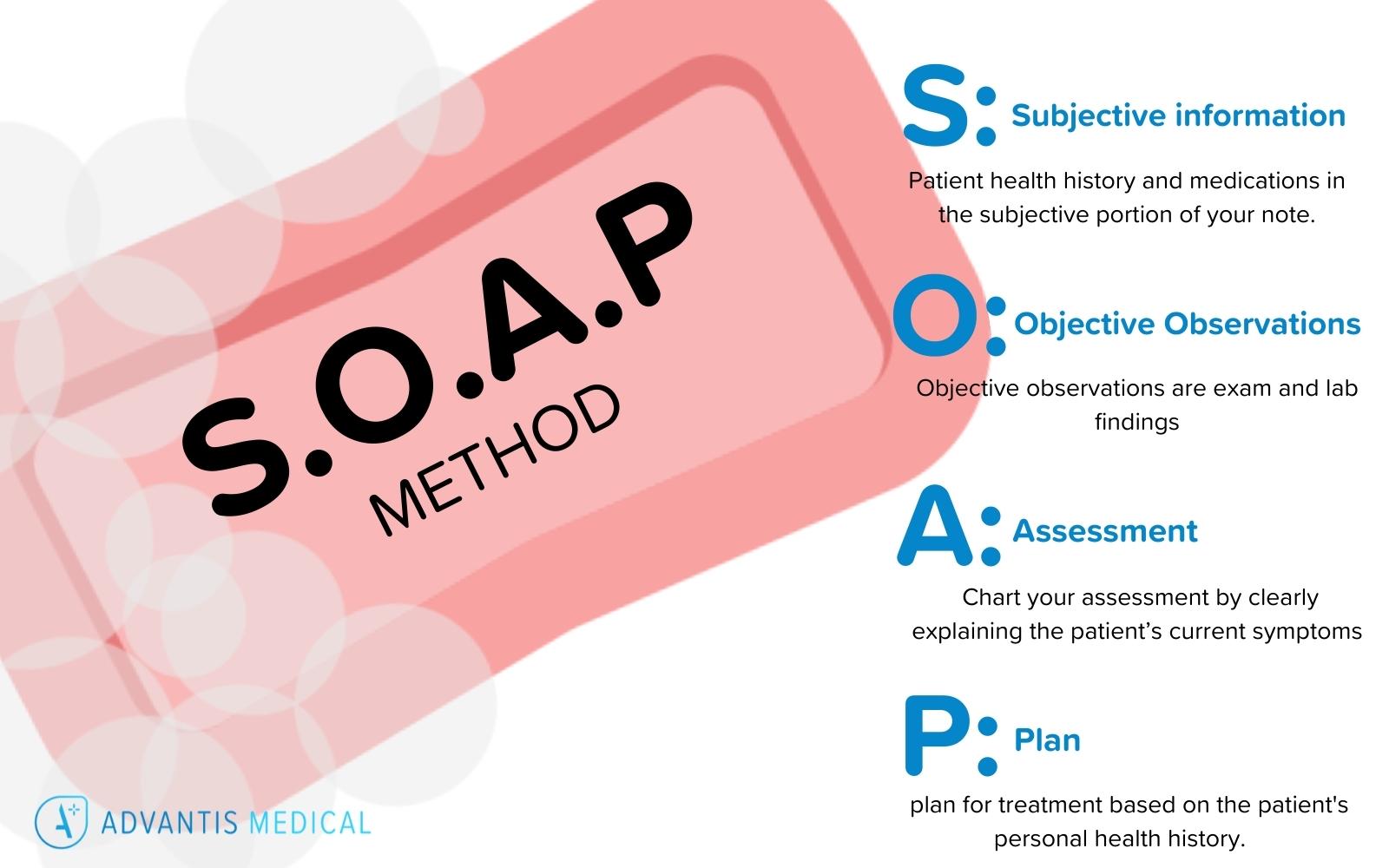
- Subjective information
- Objective observations
- Assessment
- Plan
Following the SOAP note template ensures you won’t miss anything important. You should list patient health history and medications in the subjective portion of your note. Objective observations are exam and lab findings. Chart your assessment by clearly explaining the patient’s current symptoms, then the plan for treatment based on the patient’s personal health history.
SOAP note examples
The easiest way to learn how to write a SOAP note is to review examples and practice. There are several resources for SOAP notes right at your fingertips, including Study.com, NCLEX Study Guide videos, and more. You can even view examples and use templates through carepatron.
Advantis Medical Staffing can help
Once you have some experience under your belt and you’re a nurse charting SOAP note pro, Advantis can help your career reach new heights! Our #1 rated travel nursing agency provides travel nurses and allied health professionals with exciting experiences from the emergency department to pediatrics and everything in between.
Joining our team means you can travel as much or as little as you like, with exciting experiences available across the country. Create a profile on our job portal to get started today!



